Review Course of diseases: 5 stages
The Course of Disease: 5 Stages
(Fig. 14.10)
smallpox picture

- Incubation (Table 14.9) - no symptoms : adjustment replication (bacterial infection is related to generation time of the pathogen, rabies: how close to the central nervous system)
- Prodromal- first vague symptoms (fever, malaise (yucky feeling), lack of energy, lack of appetite, very generic etc)
- Acute- recognizable, severe symptoms (vomiting and rash) picture of kid with measles and another picture of kid with small pox
- Decline-Recognizable symptoms (still there) become less severe or less frequent
- Convalescence- Symptoms gone, strength/ stamina diminished
Course
of Disease: Two Variants
R Acute disease:
Rapid onsent
Severe Symptoms: Peak of acute period has characteristic crisis point.
rapid recovery
R Chronic disease:
Delayed onset
Less severe symptoms
No crisis point, gradual transition between acute and decline
Prolonged recovery
**** drawing of graph** (example lung damage, loss of kidney may cause prolonged convalescence
*Group work: How would you draw the course of disease for malaria, which is considered a CHRONIC disease with ACUTE episodes?


*** tips on understanding how she words test questions and what she wants us to answer***
Diseases may be sequential
Timing of Diseases:
~ Primary diseases: - Occur in previously healthy individuals
~ Secondary diseases: "Piggy - back" another disease, due to immunocompromised host.
Could be another pathogen
Sequelae: could be same pathogen gaining strength or spreading to another location
**example: strep throat not treated soon enough turns into scarlet fever (toxin causes blood to leaks out into skin tissue) which can turn into Rheumatic fever damages heart tissue or post-streptococcal glomerulonephritis
http://www.medicinenet.com/strep_throat/page8.htm
~ Nosocomial disease: Fig. 14.20
* Acquired in health care setting
* MRSA: Methicillin resistant Staph. aureus
* VRE: Vancomycin resistant Enterococcus
* C. dif.: Clostridium dificile (diarrhea)
*Special considerations:
* Bad bugs there: Virulence/ drug resistance
* Immunocompromised individuals
* Many shared fomites/vehicles/ carriers
*** 40% death rate caused by nosocomial diseases for most hospitals***Location (spread) of Diseases:
u Local infection: Pathogen remains at the portal of entry (example picture skin anthrax)

u Systemic infection: Spread through system of entire body
* Septicemia: blood infection
- Bacteremia (bacteria in blood)
- viremia (virus in blood)
- fungemia (fungus in blood)
u Focal infection:
- Internal site of further spread
- Re-localization of widespread pathogen ( internal site)
*example: anthrax death cap picture brain
Pattern of Diseases in Populations:
(Epidemiology)
Endemic: (Fig. 14.16a)
* Stable predictable level over time (does not say high or low level but just stable and predictable)
Epidemic: (Fig. 14.16c)
* "outbreak" (increase of cases beyond what is expected; ex: toxic shock syndrome caused by staph aureus first described 1979... new product in 1980 super absorb tampons...left them in for 28 to 42 hours....normal flora of women's hands and if left into body for too long... high fever, pealing, sole feet, coma, death..... for menstrual women and non-menstrual women) 1980-1982
Pandemic: (Fig. 14.16d)
* Epidemic on 2 continent or more (example: 1918-1919 Spanish flu pandemic around WWI and targeted killed healthy young adults,, immune response killed them because of its strong response.. genetically similar to swine flu....).
Note: flu strains classified by location and year discovered and H and N peplomer types
graph of Rabies cases in the US (practice using words)

Diptheria cases in Independent States of Former USSR
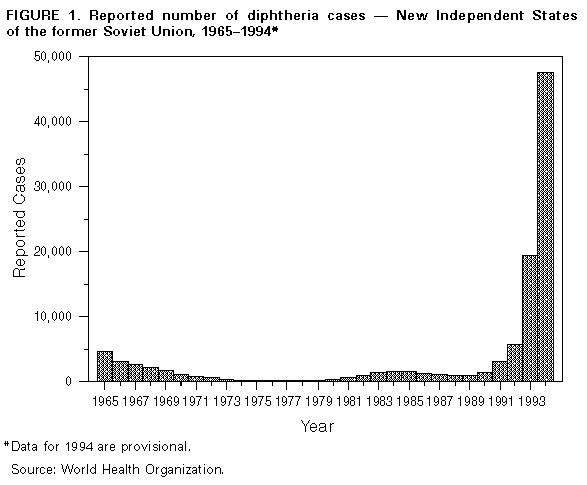
no more free available vaccines after the fall of the USSR... level of Diptheria is epidemic (or pandemic) from 1991 and beyond....
Arbovirus (mosquito-borne) cases in California:
peaks corresponding to the wet seasons in California.... 91-93 predictable = endemic
1994 = epidemic
Gonorrhea cases reported in the US

* what term describes the level of disease in 1946? what about 1976?
* give as many reasons as you can for the peaks.

http://health-fts.blogspot.com/2012/03/gonorrhea.html
**1946 WWII women work outside home, wartime 1940s... a lot more sexual activity not with regular sexual partners..
** vietnam war 1976
* why is 1976 peak so much more then 1946....social change: women burning bras, sexual revolution "make love not war" recreation drug use, birth control pill became popular (don't have to think about it as much)
1979 AIDS pandemic
**1946 WWII women work outside home, wartime 1940s... a lot more sexual activity not with regular sexual partners..
** vietnam war 1976
* why is 1976 peak so much more then 1946....social change: women burning bras, sexual revolution "make love not war" recreation drug use, birth control pill became popular (don't have to think about it as much)
1979 AIDS pandemic
*** correlated to military bases per capita *** ring of prostitutes around bases**
Types of disease: "what are you looking for?"
* Severity and progression:
* Acute versus Chronic
*when occurs (timing):
*primary versus Secondary
- Specific types of secondary = sequelae, nosocomial
Where occurs in body (location):
* local vs. systemic vs. focal
- Specific types of systemic = septicemia
- specific types of septicoma = bacteromia, viremia, fungemia
Patterns innouculations:
* Endemic, epidemic, pandemic
Types of disease: "what are you looking for?"
* Severity and progression:
* Acute versus Chronic
*when occurs (timing):
*primary versus Secondary
- Specific types of secondary = sequelae, nosocomial
Where occurs in body (location):
* local vs. systemic vs. focal
- Specific types of systemic = septicemia
- specific types of septicoma = bacteromia, viremia, fungemia
Patterns innouculations:
* Endemic, epidemic, pandemic
No comments:
Post a Comment